Transplantation of allograft extensor
Is there a solution when we have to change a prosthetic knee extensor missed?
The extensor mechanism allograft
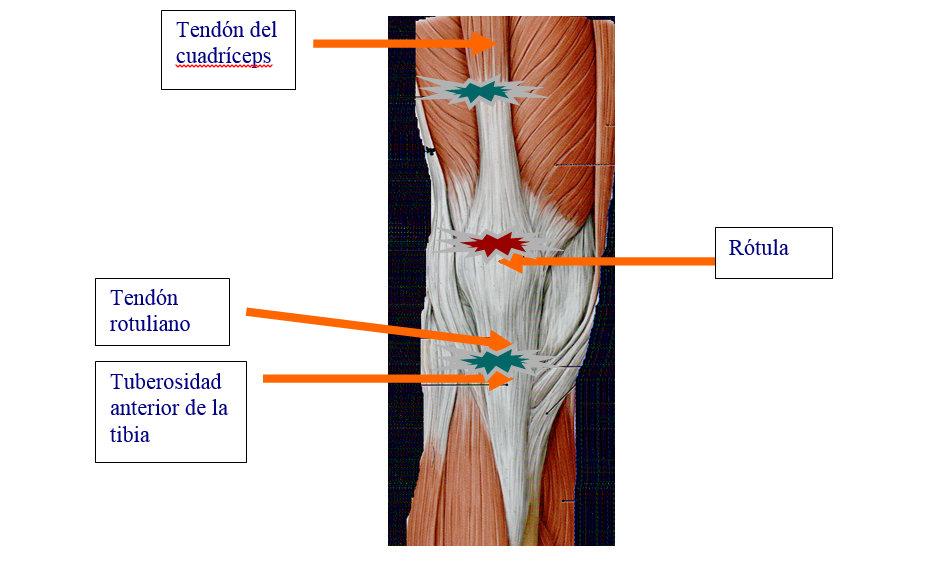
The knee extensor consists quadriceps tendon, the patella and patellar tendon. His integrity is vital for the proper functioning of the knee. Alterations in the extensor mechanism after total knee arthroplasty (PTR) They are a very difficult problem to treat. Fortunately the frequency with which they occur is low (0.17 a 2.5%).
The primary treatments, as direct sutures, fail up to 75% cases (Rand, J. A., The patellofemoral joint in total knee arthroplasty. J. Bone Joint Surg, 1994). (J. A. Rand The patellofemoral joint in total knee arthroplasty. J. Bone Joint Surg, 1994). (Rand, J.A., Total knee arthroplasty in osteonecrosis, Wink. Orthop. and Rel. True., 1991).
Well, What is this reconstruction?
The United States realized this problem. The pioneer was Emerson 1990, however suffered significant failures. In 1998, Nazarian Booth and modified the technique and succeeded in 34 of 36 cases. Last, between 2004 and 2006 Burnett sat down the pillars of the current surgery: suture tension and very strict rehabilitation protocol, including complete immobilization in a cast after surgery for about 8 the 9 weeks.
After an apprenticeship in Chicago (USA), el Dr. Andrés Camprodon Pool performed the first complete extensor mechanism allograft that has taken place in the Balearic Islands, and reconstructed knee that had lost tissue after severe infection. The operation was performed at the University Hospital in June Dureta 2006.
Extensor allograft comprises quadriceps tendon, kneecap, the patellar tendon and tibial tuberosity fragment of a donor, therefore obtained from the Tissue Bank, which is what is responsible for the safe processing and quality
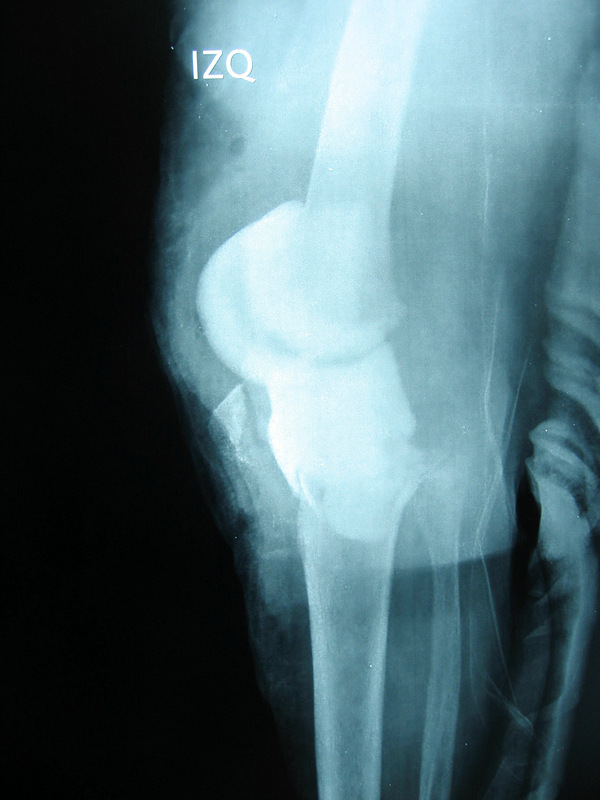 In the image on the left appreciate a snapshot of the state of the knee, the patient had been in bed more than 6 months.
In the image on the left appreciate a snapshot of the state of the knee, the patient had been in bed more than 6 months.
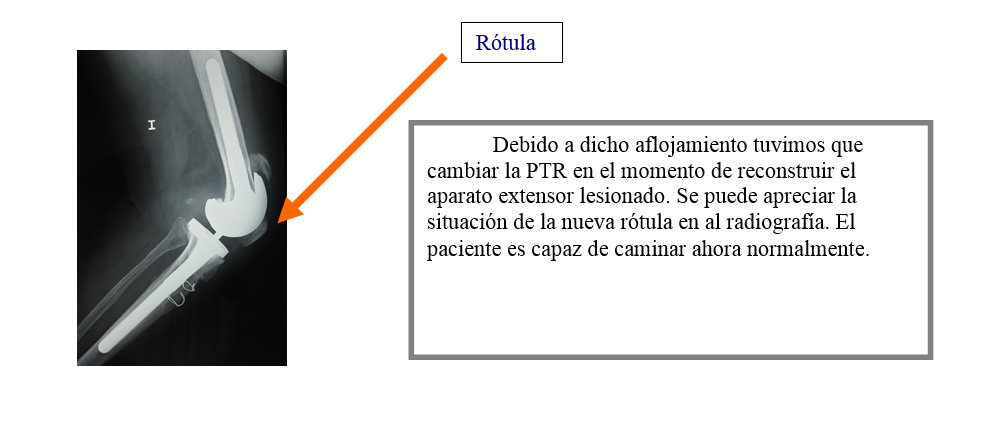
En la radiografía de la derecha se observa la nueva prótesis con el aloinjerto de aparato extensor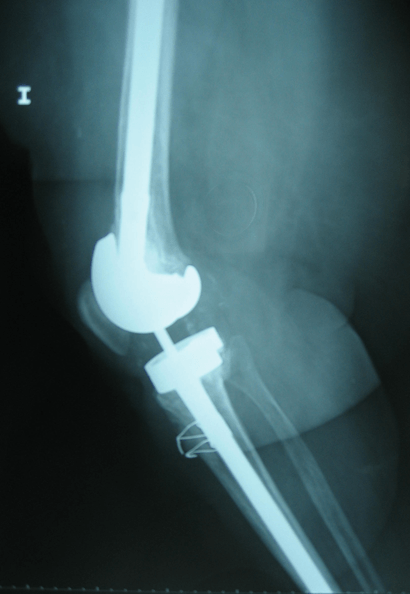
Since 2006 Dr. Camprodon successfully reconstructed knees in which many were lacking extensor. It is a very long very demanding technique that requires a learning curve, it is almost always necessary first to change the knee in the same surgical procedure.
La reconstrucción con aloinjerto de aparato extensor exige una técnica muy meticulosa, where every detail counts. Also, great difficulty to change again the old PTR is added, often in surgical scenarios such as the above image, exhibiting excessive bone loss. The arsenal of instruments to be deployed is very large, which adds difficulty to this long learning.
But, Which patients benefit from this type of surgery?
It is a very effective solution for patients who have lost the function of the extensor mechanism of the knee and are partners, assets, wanting to regain lost function and good quality fabrics. Although not all patients meet the optimum conditions because they have active infections, are too ANCIANOS TEJIDOS with the poor, or are unable to work with the strict protocol of immobilization or rehabilitation program to be practiced after this complex surgery.
Sin embargo es una solución muy eficaz para pacientes colaboradores, assets, wanting to regain lost function and good quality fabrics.